The Scourge of CKDu in Sri Lanka
What is CKDu?
The kidneys are responsible for performing several vital functions in the human body including excretion of waste products, regulation of salt and water balance, secretion of hormones and regulation of blood pressure. Several common chronic diseases such as diabetes and hypertension (high blood pressure) are known to adversely affect the health of the kidneys in the longer term. Chronic Kidney Disease of uncertain aetiology (CKDu) refers to the development of kidney disease where no discernible established cause can be found.
What may be the underlying cause of CKDu?
Several risk factors associated with CKDu have been identified, although an exact aetiology remains elusive. Most studies have found employment in the agriculture sector a risk factor, where farmers are regularly exposed to pesticides. Higher levels of agrochemicals such as glyphosate were found in drinking water and urine samples of adults living in areas where CKDu is endemic. Glyphosate is known to be nephrotoxic in animal models, most likely via an oxidative stress mechanism, which could lead to tubulointerstitial nephritis (inflammation and scarring of the kidney with progressive loss of function), one of the hallmarks of CKDu. Further support to this environmental theory comes from the clustering of individuals with CKDu that was observed around irrigation tanks and paddy fields in endemic areas of Sri Lanka.
Environmental exposure to high levels of heavy metals such as arsenic, cadmium and lead has been postulated to be a causative factor. Levels of heavy metals detected in urine samples were higher in adults with CKDu living in endemic areas. These heavy metals are present in fertilizer commonly used in paddy cultivation and significant levels have been detected in vegetables, rice and tobacco from these areas. Absorption of pesticides through skin and inhalation may occur in those employed in the agriculture sector. Excessive quantities of heavy metals present in the urine could cause oxidative damage to the kidneys.
Consumption of ground water in endemic areas appears to be associated with the development of CKDu, and this may be due to contamination of sources of water with heavy metals and agrochemicals. Genetic influences, nutritional factors, infections and recurrent dehydration have all been implicated in the causation of CKDu.
How common is CKDu in and who is affected?
The disease is not unique to Sri Lanka, with some countries in South America, the Balkans, and India reporting similar cases. In Sri Lanka, the majority of affected individuals appear to be men living in agricultural areas, with the most vulnerable age groups between 40-60 years. Prevalence rates of 2-23% have been reported in various epidemiological studies, with the North Central Province reporting the highest rates (see map below). Some studies report that the incidence of CKDu peaked in 2016 (see graph below), with estimates of more than 150,000 individuals affected across the country. It is not known whether this increase in incidence was due to better case detection from screening programmes initiated by the health services, or a true increase in disease incidence due to an unidentified aetiological factor. The observed reduction in CKDu incidence in 2017 was attributed to the provision of safe drinking water in affected areas by some investigators.
The diagnosis of CKDu leads to significant disability with profound socioeconomic implications for patients and their families. Around 30% of adults with CKDu die within 5 years of diagnosis.
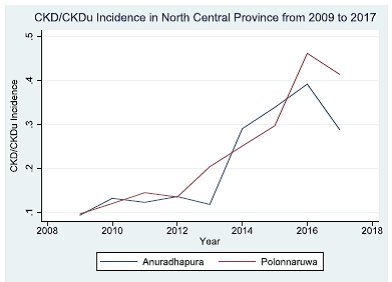 Trend in incidence of CKDu in Sri Lanka | 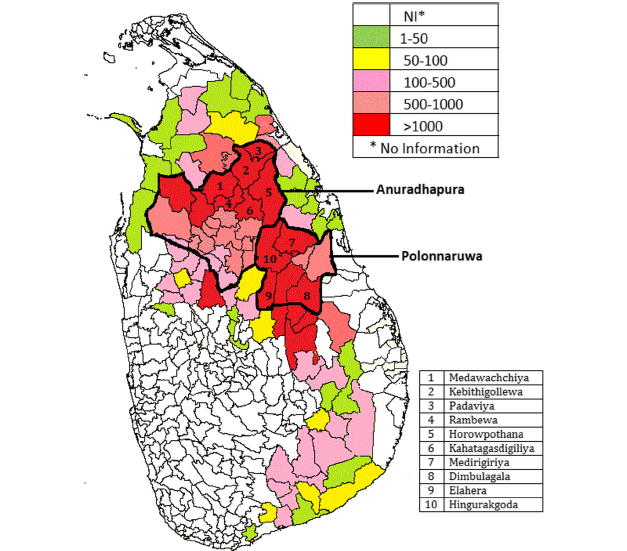 Geographical distribution of CKDu |
What symptoms do people have?
The majority of individuals do not report any symptoms in the early stages of the disease. This makes CKDu particularly difficult to manage as patients present to health services with advanced irreversible damage to their kidneys. With such advanced kidney disease, patients may experience anorexia, nausea, limb swelling, fatigue, breathlessness, itching, reduced urine output and confusion.
How is CKDu diagnosed?
It is difficult to distinguish between CKDu and other causes of CKD from clinical assessment only. The diagnosis would depend on excluding other known causes of CKD such as pre-existing hypertension and diabetes, and eliciting occupational and environmental risk factors discussed previously. Increased excretion of protein (proteinuria) and impaired kidney function demonstrated using blood tests, are some of the principal features seen in CKDu. These tests can be used in screening programmes in CKDu endemic areas. Imaging of the kidneys using ultrasound scanning may show bilaterally small kidneys. Kidney biopsies from adults with CKDu may show evidence of scarring (fibrosis), inflammation and wasting of kidney cells (atrophy).
What treatment options are available?
There are no specific guidelines for the treatment of CKDu. General treatment strategies used for the management of chronic kidney disease due to other established causes are instituted. These include managing other coexisting conditions that may occur such as diabetes and hypertension which would further contribute to the decline in kidney function; treating with medication that may halt the progression of kidney disease; managing complications such as heart disease that these patients are more likely to develop; preventing osteoporosis (thinning of bones); managing malnutrition; and stopping smoking. Some patients who develop ‘end-stage’ CKDu will be offered renal replacement therapy, commonly referred to as ‘dialysis’.
Removal of exposure to potential environmental toxins discussed previously may help with preventing disease progression, but further studies to confirm this are needed.
What does the future hold for CKDu in Sri Lanka?
The majority of patients with CKDU do not display symptoms initially, and the disease progresses insidiously. There are currently no specific treatment options available for the management of CKDu. Therefore considerable attention has been focused on early detection of patients with CKDu. Screening programmes in CKDu endemic areas using a combination of blood tests and urine tests should allow identification of individuals with early disease, allowing prompt intervention. Several additional bio markers for the detection of CKDu have been investigated in studies, but their utility in routine practice has been limited due to cost and lack of effectiveness.
Once detected, patients with CKDu require access to renal clinics where their condition could be monitored for progression, and treatment initiated to prevent complications. Those who go on to require renal replacement therapy need access to dialysis clinics for regular treatment sessions and management of dialysis related complications. All of this requires further development of the infrastructure of renal services in Sri Lanka, streamlining resources and adequate allocation of funding at the national level, particularly to some rural areas where CKDu is endemic. Strategies to minimise exposure to the risk factors associated with CKDu should be implemented more widely. The World Health Organisation recommends the provision of safe drinking water and undertaking adequate safety precautions in the agricultural sector in Sri Lanka. The successful implementation of such strategies also depends on stringent education programmes, held at regular intervals, aimed at the general public and healthcare workers to increase their awareness of CKDu.
Despite a large amount of high quality research conducted in Sri Lanka over the past few years in relation to CKDu, significant gaps in our knowledge still remain. Further research in to current epidemiological trends, causative factors, methods of screening, and disease management is urgently needed to halt the scourge of CKDu in Sri Lanka.
Article by : Dr Chamira Rodrigo BM(Hons) BSc(Hons) MRCP PhD Consultant Physician in Respiratory Medicine and General (Internal) Medicine Nottingham University Hospitals NHS Trust
References
- Redmon J, Elledge M, Womack D, et al. Additional perspectives on chronic kidney disease of unknown aetiology (CKDu) in Sri Lanka–lessons learned from the WHO CKDu population prevalence study. BMC Nephrol. 2014 Jul 28;15:125. doi: 10.1186/1471-2369-15-125.
- Rajapakse S, Shivanthan MC, Selvarajah M. Chronic kidney disease of unknown etiology in Sri Lanka. Int J Occup Environ Health. 2016 Jul;22(3):259-264. doi: 10.1080/10773525.2016.1203097. Epub 2016 Jul 11.
- Rajapakse S, Shivanthan MC, Selvarajah M. Chronic kidney disease of unknown etiology in Sri Lanka. Int J Occup Environ Health. 2016 Jul;22(3):259-264. doi: 10.1080/10773525.2016.1203097. Epub 2016 Jul 11.
- Ratnayake S, Badurdeen Z, Nanayakkara N, et al. Screening for chronic kidney disease of uncertain aetiology in Sri Lanka: usability of surrogate biomarkers over dipstick proteinuria. BMC Nephrol 18, 199 (2017) doi:10.1186/s12882-017-0610-x
- Wijkström J, Jayasumana C, Dassanayake R et al. Morphological and clinical findings in Sri Lankan patients with chronic kidney disease of unknown cause (CKDu): Similarities and differences with Mesoamerican Nephropathy PLOS ONE 13(3): e0193056
- Ranasinghe A, Kumara G, Karunarathna R, et al. The incidence, prevalence and trends of Chronic Kidney Disease and Chronic Kidney Disease of uncertain aetiology (CKDu) in the North Central Province of Sri Lanka: an analysis of 30,566 patients. BMC Nephrol. 2019;20(1):338. Published 2019 Aug 28. doi:10.1186/s12882-019-1501-0